JAVNI IZDACI ZA ZDRAVSTVO U EVROPSKOJ UNIJI PRE, TOKOM I NAKON PANDEMIJE COVID-19

Apstrakt
Pandemija COVID-19 predstavljala je najveći izazov za zdravstvene sisteme Evropske unije u novijoj istoriji, dovodeći do značajnih promena u obimu i strukturi javnih izdataka za zdravstvo. Ovaj rad analizira javnu zdravstvenu potrošnju u zemljama Evropske unije pre, tokom i nakon pandemije (2015–2024), sa ciljem identifikovanja ključnih trendova, razlika među državama članicama i dugoročnih implikacija za finansiranje zdravstvenih sistema.
Istraživanje pokazuje da je pandemija dovela do privremenog, a u pojedinim slučajevima i trajnog povećanja zdravstvenih izdataka, istovremeno podstičući niz reformi usmerenih na jačanje otpornosti zdravstvenih sistema. Ipak, održivost povećanih budžetskih izdvajanja ostaje izazov, naročito u kontekstu fiskalne stabilnosti.
Rad zaključuje da je adekvatno finansiranje ključno za dugoročnu otpornost zdravstvenih sistema i nudi preporuke za unapređenje politika finansiranja u postpandemijskom periodu.
Članak
Introduction
Public health expenditure represents the total amount of financial resources allocated by government authorities (central and local levels of government) to finance the health system, including hospital services, primary health care, preventive programs, public health campaigns and other activities aimed at preserving and improving the health of the population. According to the World Health Organization (WHO), public health expenditure includes “all payments for health care that originate from public sources, regardless of whether the costs are incurred directly through public institutions or indirectly through public funds and insurance” (WHO, 2022). Reeves et al. (2022) state that public health expenditure is a key instrument by which governments ensure access to health services, control health costs and influence the health outcomes of the population, especially in crisis situations such as the COVID-19 pandemic. In the domestic literature, Ćulibrk (2021) emphasizes that public health spending in Serbia and other countries in the region is financed primarily from mandatory health insurance and budget funds, and that “the level of spending needs to be approached systematically, taking into account both the effects on health and the sustainability of public finances”. Within the European Union, public health spending is usually expressed as a percentage of GDP or per capita, which allows for comparison between member states.
Sufficient and stable health spending is the foundation of an efficient and sustainable health system. According to OECD (2022), health systems with higher levels of public spending achieve better results in terms of service availability, life expectancy and patient satisfaction. Public spending enables continuous financing of health institutions, the purchase of medical equipment, human resource development and the introduction of new technologies. The World Health Organization (WHO, 2022) emphasizes that increased public health spending has a direct impact on reducing financial barriers for patients, thereby contributing to more equitable access to health care. Also, adequate financing is crucial for strengthening preventive programs and the resilience of the system to emergencies, such as the COVID-19 pandemic. In the European context, Rajan et al. (2021) emphasize that it is precisely those countries that invested in health before the pandemic that have shown greater readiness to respond to the crisis, both in terms of hospital capacity and staff stability and availability of basic health care. In the domestic literature, Simić et al. (2020) indicate that in Serbia, insufficient allocations to health represent a limitation in the development of health services and improving the quality of treatment. The authors particularly emphasize that investments in primary health care and staff are necessary for the long-term stability of the system. From an economic point of view, health allocations are considered not only a cost, but also an investment in human capital, which stimulates economic growth, reduces disease rates and prolongs the working capacity of the population (Fattore & Tediosi, 2022).
The COVID-19 pandemic has dramatically tested the resilience of health systems in the European Union, pointing to structural weaknesses but also the potential for adaptation and reform. According to research by Rajan et al. (2021), health systems in the EU have been under immense pressure due to hospital overcrowding, shortages of health workers, and limited supplies of protective and medical equipment. The research highlights that even highly developed countries such as Italy and Spain have been forced to take extraordinary measures, including mobilizing the private sector and military logistics. As Anderson et al. (2022) point out, the pandemic has exposed disparities in public health capacities and shown that systems that invested in preventive measures and public health were better prepared to manage the crisis. In this context, northern and Scandinavian countries have generally had a more effective response compared to countries in southern Europe. The OECD report (2022) states that the pandemic has led to a significant increase in public health spending in all EU member states. Most countries have adopted aid packages and introduced extraordinary funding to strengthen hospital capacity, testing, vaccination, and the digitalization of health services. At the domestic level, Ćulibrk (2021) states in his analysis that the pandemic represented "a catalyst for rapid response, but also the discovery of chronic problems", such as inadequate infrastructure, outdated equipment and insufficient staffing. He particularly emphasizes the role of crisis headquarters, but also the need for a more systematic approach to health financing. In addition to the direct impact on health infrastructure, the pandemic also affected the availability of regular health services. According to the European Commission (2021), many countries have recorded a decline in the number of preventive examinations, surgical interventions and treatment of chronic diseases, which may have long-term consequences for the health of the population.
The main objective of this paper is to analyze the volume, structure and trends of public health spending in the European Union countries during and after the COVID-19 pandemic. The paper aims to highlight changes in the level of health spending, differences between member states, as well as the impact of these changes on the functioning and resilience of health systems. Special attention is paid to the analysis of the long-term sustainability of increased spending, the reforms that followed, as well as recommendations for improving the financing of health systems in the future.
The methodology of the paper is based on a combination of qualitative and quantitative analysis. The following methods were used in the paper:
-
Analysis of secondary data: official statistics from Eurostat, OECD, WHO, as well as data from national institutions;
-
Review of relevant literature: scientific and professional papers, reports, publications of international organizations;
-
Comparative analysis: comparison between Western and Eastern European countries;
-
Graphical and tabular presentation of data: for easier interpretation of the results;
-
Synthesis of findings: with the aim of identifying long-term implications and formulating recommendations.
Theoretical framework of public health spending
Public health spending represents financial allocations from public sources – state, regional and local budgets, as well as mandatory health insurance – used to finance health services, infrastructure and public health measures. It includes costs covered by governments and public institutions, as well as public health insurance funds, and is a key instrument of the state in ensuring the availability and quality of health care (OECD, 2021). According to the World Health Organization (WHO, 2022), public health spending includes all costs covered by public sources, regardless of whether services are provided in public or private institutions. This spending is the basis for the functioning of the health system, as it allows for the financing of salaries of health workers, the purchase of medicines, medical equipment, investment in infrastructure, but also in public health activities such as vaccination and health education.
The main components of public health spending include:
-
Primary health care – health centers and family medicine (WHO, 2022; Simić et al., 2020).
-
Secondary and tertiary care – hospital services, specialist treatment and surgery.
-
Public health – preventive measures, immunisation, control of communicable diseases and health promotion (OECD, 2022).
-
Health administration and support – system management costs, staff training, information systems.
-
Infrastructure and investment – construction and renovation of health facilities, investment in equipment and technology.
According to the OECD classification (SHA – System of Health Accounts), public financing of health can be measured as:
-
Share of total health expenditure (%),
-
Amount per capita (in euros),
-
Share of GDP (%), which allows comparison between countries and assessment of the priorities that the state gives to health (OECD, 2021).
To analyse and compare health expenditure between countries and over time, standardised health expenditure indicators are used. These indicators allow decision-makers, researchers and international institutions to monitor the efficiency and equity of health system financing, but also to identify trends and potential risks. According to the OECD (2021) and the World Health Organization (WHO, 2022), the most important indicators of health spending are:
-
Public health spending as a percentage of GDP (% GDP) - This indicator measures the share of public spending on health in relation to the country's gross domestic product. A higher percentage indicates a higher priority for health within public policies. The EU average in 2021 was around 8% of GDP (Eurostat, 2023).
-
Health spending per capita (in euros or dollars, adjusted for PPP) - It represents the total public and private spending on health per person. According to OECD (2022), this indicator is often used to assess the availability and quality of health services. Differences between countries can be very pronounced – from less than €1,000 in some Eastern European countries to over €5,000 in Western European countries.
-
Share of public expenditure in total health expenditure (%) - Measures the proportion of total expenditure financed by public sources compared to private sources, including co-payments and private insurance. A higher share of public expenditure indicates a greater role of the state in financing health and a lower financial burden on citizens (WHO, 2022).
-
Out-of-pocket expenditure (direct payments by patients) as a percentage of total expenditure - According to the WHO, this indicator is an important indicator of the financial protection of citizens. A high share of direct payments may indicate an inefficient or insufficiently solidarity-based system (Reeves et al., 2022).
-
Structure of spending by function and type of service - In accordance with the OECD System of Health Accounts (SHA), allocations are analyzed by function (e.g. hospital care, prevention, outpatient services) and by type of financier (public, private, mandatory insurance) (OECD, 2021).
The financing of health systems in the European Union is primarily the responsibility of national states, which means that each member state independently defines the model of organization, scope and structure of public health spending. The European Union as a whole does not have the competence to directly manage health systems, but acts through coordination, recommendations and support through programs such as EU4Health or RescEU (European Commission, 2022). According to data from the OECD (2021) and WHO (2022), the dominant model in most EU countries is the public financing model, which is based either on taxation (the so-called Beveridge model), as in Sweden and Spain, or on mandatory health insurance (the so-called Bismarck model), as in Germany, France and Austria. These models are often combined with various solidarity mechanisms and complementary private funds.
Member States play a key role in ensuring stable and equitable financing of health, through:
-
Adopting the annual health budget,
-
Price regulation and reimbursement of medicines and health services,
-
Infrastructure investment planning,
-
Subsidizing vulnerable groups (elderly, unemployed, chronic patients).
As Reeves et al. (2022) emphasize, during and after the COVID-19 pandemic, the role of member states has become even more pronounced in the context of increasing public spending, accelerating the introduction of digital services, and better managing health risks. The crisis has shown that flexibility in budgeting and centralization of decisions have contributed to a faster response in most countries. In the domestic literature, Simić et al. (2020) emphasize that the role of the state in healthcare financing is not only in providing funds, but also in determining priorities and fairness of distribution. The authors indicate that in Serbia, as in many EU countries, state intervention has a decisive impact on the accessibility and quality of services. It is important to note that although Member States have primary responsibility, the EU is increasingly supporting data integration, cross-border cooperation and common policies in areas such as rare diseases, digital health and health risks (European Commission, 2022).
Public spending on health in the EU before the pandemic (2015–2019)
The period before the COVID-19 pandemic, i.e. the years from 2015 to 2019, was characterized by relative stability in the financing of health systems in the European Union. Although health expenditure grew at a moderate pace, there were significant differences between countries in terms of absolute amounts, cost structures and investment priorities. According to data from the OECD (2020) and Eurostat (2020), average public spending on health in EU countries during this period amounted to around 7.8% of GDP, with a slight upward trend. Health expenditure per capita increased from an average of €2,500 in 2015 to around €3,000 in 2019, adjusted for purchasing power parity (PPP). The highest public spending as a percentage of GDP in 2019 was recorded in: France (9.3%), Germany (9.1%), Sweden (9.0%). On the other hand, a significantly lower share of public expenditure in GDP was recorded in: Romania (5.0%), Bulgaria (4.7%) and Latvia (5.4%), which indicated the still existing inequalities in the availability and quality of healthcare within the Union (WHO, 2019). Eurostat (2020) indicates that during this period, health budgets in most Member States were used primarily for: hospital services (40–50% of public expenditure), outpatient care and specialist examinations, medicines and medical devices, preventive measures and public health (which, on average, accounted for less than 3% of total expenditure). According to research by Reeves et al. (2019), before the pandemic there was no significant increase in investment in public health infrastructure and systemic preparedness for health crises, which became clearly visible during the COVID-19 pandemic. In the domestic context, Simić et al. (2018) state that Serbia, as a non-EU country but a candidate for membership, invested around 5.3–5.5% of GDP in the health sector during this period, which was below the European average. The authors point out that the dominant part of spending was directed at secondary and tertiary care, while the preventive segment was underestimated. Despite the relatively stable growth of public health expenditure in the EU in the period 2015–2019, it was observed that there was insufficient systematic approach to preparing for pandemic risks, and the COVID-19 pandemic highlighted the need for greater and faster investments in the resilience and flexibility of health systems (OECD, 2021).
Before the onset of the COVID-19 pandemic, one of the most significant characteristics of health financing in the European Union was the pronounced inequality between Western and Eastern member states. These differences were reflected both in the absolute amounts of public spending, as well as in its structure, system efficiency and health care outcomes. According to Eurostat (2020), Western European countries such as Germany, France, Belgium and the Netherlands spent between 9 and 10% of GDP on health, while Eastern member states such as Bulgaria, Romania, Latvia and Lithuania spent significantly less — between 4.5 and 6% of GDP. In addition to the percentage of expenditure in relation to GDP, there was also a significant difference in per capita spending. For example, in 2019, public spending on health per capita in Germany was around €5,000, while in Romania it was less than €600 (OECD, 2020). These differences further deepened the gap in access to and quality of health services. Reeves et al. (2019) indicate that Eastern countries, despite smaller budgets, often face greater challenges in terms of demographic pressures (aging population, migration of health workers) and lower efficiency in the allocation of resources. In addition, investments in prevention and public health were proportionally lower in Eastern European countries, which contributed to higher levels of avoidable disease and mortality. WHO (2019) and OECD (2018) point out that Western members generally had: more developed infrastructure and digitalization of healthcare, better capacity of hospital systems (in terms of equipment and staff), more stable financing mechanisms and cost control. On the other hand, Eastern countries often depended on a health insurance model based on employment status, which led to instability in times of economic crises. Also, the lack of investment in human resources led to a massive outflow of medical staff to Western countries, which further undermined capacities (Simić et al., 2018). Simić and Petrović (2019) emphasize in the domestic literature that Serbia, although outside the EU, is part of the same trend of uneven and structural insufficiency of financing, with significant reliance on out-of-pocket payments from patients and insufficient budgetary space for innovation. Overall, the differences between Western and Eastern Member States in the financing of health systems before the pandemic reflected broader economic inequalities, but also differences in the priorities and capacities of public administration.
The financing of health systems in the European Union is based on different models, but essentially relies on three main sources: public funds (budgetary and social security), private insurance and direct payments from citizens' pockets. The structure of these sources varies significantly between Member States, depending on the organization of the system, economic development and policies social protection.
According to the classification of the OECD (2017) and WHO (2019), the two dominant models in the EU are:
-
Beveridge model – financing through tax revenues (examples: Great Britain, Sweden, Denmark)
-
Bismarck model – financing through contributions to compulsory health insurance (examples: Germany, France, Austria)
Accordingly, the main sources of health financing in most EU countries are:
-
Public funds (government and compulsory insurance): On average, public sources accounted for around 75–80% of total health expenditure in most EU countries in the period 2015–2019 (Eurostat, 2020). In countries such as Sweden, Norway and the United Kingdom, this percentage even exceeded 85% (OECD, 2020).
-
Out-of-pocket payments: On average, they accounted for 15–20% of total spending, but in Eastern Member States such as Bulgaria, Latvia and Romania they often exceeded 30% (WHO, 2019). These expenditures most often relate to the purchase of medicines, dental services and long-term care (Reeves et al., 2019).
-
Voluntary health insurance: The share ranged from 1% to 13% depending on the country (Eurostat, 2020). It is most common in France and the Netherlands, where it serves as a supplementary mechanism for covering co-payments or additional services.
Mossialos et al. (2018) indicate that a combination of public insurance and supplementary policies is the most common approach in Bismarckian model countries. On the other hand, Eastern European countries often do not have a developed voluntary insurance market, which results in a higher fiscal burden on citizens. In the domestic literature, Jovanović et al. (2018) point out that in Serbia the dominant source of financing is the RFZO (Republic Health Insurance Fund), which is financed by contributions from salaries, while about 35% of costs are financed from patients' pockets, which indicates a similar trend as in some eastern EU member states. In general, differences in sources of financing significantly affect the availability and equality of use of health services. Countries with a higher share of public expenditure tend to achieve better results in terms of access, financial protection and health outcomes (WHO, 2019).
Public spending on health in the European Union before the COVID-19 pandemic was structured to cover different types of services, with the largest part of the budget being directed to hospital care, outpatient services and medicines. The structure of this spending reflects the organizational models, priorities of health systems, but also the demographic and epidemiological needs of the population.
According to OECD (2019) and Eurostat (2020), the average structure of public spending in the EU was as follows:
-
Hospital care – accounted for 30–40% of total public spending. This category includes inpatient care, surgery, emergency care and specialized hospital care. Countries such as Germany and Austria had a strong concentration of spending in this segment, given the large number of hospital capacities (WHO, 2019).
-
Outpatient care – accounted for 20–25% of spending, including primary health care, specialist examinations and diagnostic services. In countries such as the Netherlands and Sweden, where primary health care is highly developed, outpatient services played a larger role in the system (Mossialos et al., 2018).
-
Pharmaceuticals and medical goods – accounted for 15–20% of the total public health budget. Differences between countries are significant – in the Eastern Member States, spending on medicines was often higher than in other segments, due to the smaller volume of other public services (Reeves et al., 2019).
-
Long-term care – accounted for 8–15% of total spending, with countries with older populations such as Finland and France investing more in this type of service. According to WHO (2018), investment in long-term care was insufficient in most of the Eastern Member States.
-
Prevention and public health – accounted for 3–5% of the budget, with a higher share in the Scandinavian countries. Despite prevention being key to reducing the burden of disease, this segment was chronically underfunded in most countries (OECD, 2019; WHO, 2019).
-
Administration and support of the system (health administration and governance) – accounted for 2–4% of total expenditure. - In the domestic literature, Pejić and Matić (2017) point out that the structure of health spending in Serbia, which has similarities with the eastern EU member states, showed an excessive focus on hospital treatment and medicines, while neglecting preventive and primary care services. WHO (2019) specifically emphasizes that the unevenness in the structure of spending is the result not only of financial capacities, but also of different policies for the development of health systems. Countries that invested more in primary care and prevention had better health outcomes and lower total spending per capita.
Impact of the COVID-19 pandemic on public health spending in the EU
The COVID-19 pandemic has significantly changed the fiscal priorities of EU Member States, leading to a sudden and large-scale increase in public health expenditure. According to OECD (2021), in 2020, almost all EU Member States increased their health budgets to respond to the immediate needs caused by the pandemic – from the procurement of medical equipment and tests, to investments in hospitals and intensive care, to the financing of vaccination campaigns.
According to Eurostat (2022), average public spending on health in the EU increased from 7% of GDP in 2019 to over 8% in 2020, which is the largest annual increase in the history of available data. In France and Germany, public health expenditure reached over 11% of GDP, while in Spain it increased from 6.4% to 7.8% of GDP over the same period (OECD, 2021; WHO, 2021). In the study by Mladovsky et al. (2022) highlights that the main components of the increase were: increased salaries and bonuses for healthcare workers, investments in ventilators, tests, PPE (personal protective equipment), expenditures for hospital capacities and intensive care units, the introduction of mass vaccination programs, state interventions and extraordinary investments. Many member states have introduced extraordinary funds and packages to support healthcare. For example, Italy allocated over 9 billion euros additionally to the healthcare sector in 2020 (Italian Ministry of Economy and Finance, 2021), Germany established a special fund of over 20 billion euros to combat COVID-19 and support hospitals (BMG, 2021), and Slovenia increased the budget of the Ministry of Health by 40% compared to 2019 (SURS, 2022).
According to domestic authors, Stanković and Kovačević (2021) indicate that the pandemic served as a catalyst for “rapid and extraordinary mobilization of resources” and revealed structural weaknesses in healthcare systems in the region, which required additional public investments.
According to the WHO Regional Office for Europe (2021), the increase in public health spending has in many cases been financed by borrowing or budget rebalancing, which raises the question of fiscal sustainability in the future.
The COVID-19 pandemic has forced European Union countries to quickly adjust their fiscal and health policies. The response has included a range of temporary (ad hoc) measures, but also long-term structural interventions aimed at strengthening health systems and their resilience. According to the WHO (2021) and OECD (2022) reports, most EU countries have taken the following temporary measures in 2020–2021: the establishment of emergency funds for emergency procurement (respirators, PPE, tests), additional funding for hospitals and expansion of intensive care capacity, financial incentives for health workers, including bonuses and salary increases, rapid subsidies to private providers who were engaged in the COVID system, the introduction of mass vaccination programs with centralized procurement and financing at the national level (European Commission, 2021). In the same context, Reeves et al. (2022) point out that in Germany, for example, a special fund Sondervermögen was established, which financed healthcare, the economy and the procurement of vaccines worth over 30 billion euros.
Although a large part of the measures were temporary in nature, the pandemic also encouraged the adoption of long-term measures and strategies, such as: increasing the base budget for healthcare in the next budget cycles, investing in the digitalization of the healthcare system (e-health, e-cards, telemedicine), strengthening primary and preventive healthcare, strategic construction of new facilities and modernization of old hospitals, employment and additional education of healthcare workers (OECD, 2023; Pajić et al., 2025). The EU4Health 2021–2027 program, which the European Commission launched in response to the pandemic, provided a budget of 9.4 billion euros, which is the largest amount in the history of the EU dedicated to healthcare. The objectives of this program include building health resilience, better cross-border cooperation and preparation for future crises (European Commission, 2021). In the domestic context, Kovačević et al. (2021) note that in Serbia, although temporary measures (e.g. crisis funds, budget rebalancing) prevailed, the pandemic nevertheless spurred plans to invest in digitalization and the renovation of hospital infrastructure through multi-annual investment programs. WHO (2021) points out that one of the positive outcomes of the crisis is that “health has finally become a central theme of fiscal policy in many countries”, which could influence the long-term increase and better structure of public spending. During the COVID-19 pandemic, the European Union played a key role in financing the health systems of member states. Through funds such as EU4Health (worth €9.4 billion) and NextGenerationEU, the EU provided funds for the procurement of medical equipment, the development of vaccines, the strengthening of health infrastructure and the digitalization of services (European Commission, 2022; WHO, 2021). At the same time, member states have introduced temporary measures (bonuses for medical workers, free tests and treatment, construction of temporary capacities), but have also begun long-term investments in healthcare — increasing wages, strengthening staff, modernizing hospitals and transitioning to digital health systems (OECD, 2021; Ministère de la Santé, 2021). During the COVID-19 pandemic, the European Union adopted several instruments to support the health systems of member states, giving health policy a prominent place within the common budget and solidarity mechanisms for the first time.
-
EU4Health Programme (2021–2027)
The most important EU health instrument during and after the pandemic is EU4Health, which is a response to the systemic weaknesses of health systems identified during the crisis. With a budget of €9.4 billion, this programme has financed:
-
procurement of medicines, vaccines and medical equipment,
-
cross-border cooperation in combating infections,
-
strengthening human capacity and digitalisation of systems,
-
better preparedness for future health threats (European Commission, 2021).
As Greer et al. (2022) state, EU4Health marked “a historic turning point in the EU’s approach to health, moving from coordination to active financing”.
2. NextGenerationEU and the Recovery and Resilience Facility (RRF)
In addition to direct health funds, the European Union has adopted the largest economic package in its history through the NextGenerationEU mechanism — over €800 billion, a significant part of which is intended to strengthen the resilience of public systems, including healthcare.
As part of this package, the Instrument for Recovery and Resilience (RRF) has financed:
-
construction of new hospital capacities,
-
improvement of primary healthcare,
-
digital reforms (e-health, e-cards) in several countries, such as Portugal, Italy and Greece (OECD, 2022; Mladovsky et al., 2022).
3. Solidarity Fund and Civil Protection Mechanism
Through the EU Solidarity Fund, several countries (including Italy, Spain and Romania) have received financial assistance for emergency measures such as the procurement of protective equipment, support to hospitals and the evacuation of patients (European Court of Auditors, 2021). Also, rescEU — the EU civil protection mechanism — financed common stocks of medical equipment (respirators, vaccines, PPE) and established logistical support across the Union.
4. Effects in Serbia and candidate countries
Although not a member of the EU, Serbia received significant funds under the Instrument for Pre-Accession Assistance (IPA III) to combat the pandemic. According to Kovačević et al. (2022), over 15 million euros of EU support was used for medical equipment, testing and support to the most vulnerable categories of the population.
The role of the European Union in financing healthcare during the COVID-19 pandemic was multifaceted, encompassing direct investments, loans and grants, as well as the development of institutional resilience. This intervention laid the foundation for further integration of health policies within the Union.
The COVID-19 pandemic led to a sharp increase in public spending in all European Union countries, but the volume and structure of these allocations varied significantly depending on economic strength, the organization of the healthcare system and the degree of impact of the virus. According to OECD (2021) and Eurostat (2022), the average level of public health expenditure in the EU increased from 7.0% of GDP in 2019 to 8.0% of GDP in 2020, the largest relative increase in recent decades. Countries with strong economies and developed health systems, such as Germany, France, Sweden and the Netherlands, achieved the largest absolute and relative increases in health spending. Germany increased its total public health spending from 11.7% to 12.8% of GDP in 2020 (Statistisches Bundesamt, 2021). France allocated more than €20 billion for emergency health interventions, including bonuses for medical staff and financing of hospital capacities (Ministère de la Santé, 2021). Sweden increased its funding of regional health authorities by over 25% compared to 2019 (OECD, 2021).
Eastern European EU member states — such as Bulgaria, Romania, Hungary and Croatia — also increased public spending on health, but from a significantly lower base. In Bulgaria, public health expenditure increased from 4.1% to 5.0% of GDP (Eurostat, 2022). In Romania, despite an increase of more than 30% in nominal terms, spending remained below the EU average, at 6.1% of GDP (Mihaila & Popescu, 2022). Croatia largely covered the increased costs from EU funds and loans through the EIB and EBRD (Ministry of Health of the Republic of Croatia, 2021).
While Western countries invested more in infrastructure (hospital renovation, intensive care units), vaccine development and ICT solutions (e-health), Eastern member states prioritized the procurement of protective equipment and tests, support for primary health care and temporary employment of additional medical staff (Karanikolos & Mossialos, 2020).
In 2020, public health expenditure per capita amounted to:
-
Germany: around 5,700 euros
-
France: 5,100 euros
-
Sweden: 5,400 euros
-
Hungary: 1,500 euros
-
Romania: 1,200 euros
-
Bulgaria: below 1,000 euros (OECD, 2021; Eurostat, 2022)
These differences indicate a continuing gap in funding and capacity between the Western and Eastern parts of the EU.
Public health spending after the pandemic
In the post-COVID-19 period (2022–2024), public health expenditure in the European Union has shown a number of new trends, reflecting the transition from emergency financing to a sustainable health system, while also facing inflation, an ageing population and staff shortages. According to Eurostat (2023), the share of public health expenditure in GDP in 2022 fell in most Member States, after peaking during the pandemic. The EU average was 8.1% of GDP, down from 8.5% in 2021. The largest decreases were recorded in Bulgaria (-1.1 percentage points), Hungary and Lithuania (-0.9 pp), while Luxembourg and Slovenia showed a slight increase (Eurostat, 2023). These trends are also confirmed by the OECD (2023), which states that in the member countries of this organization the share of health expenditure in GDP fell from 9.7% in 2021 to 9.2% in 2022, due to the cessation of pandemic programs and the effects of inflation on nominal GDP. Although the overall share of health expenditure in GDP has declined, in many countries absolute costs have remained high or even increased. For example, in Estonia in 2023 health expenditure remained at the level of 7.5% of GDP, similar to the pandemic years, which is the result of a significant increase in the salaries of health workers (WHO, 2023a). The salaries of doctors and nurses in this country have increased in the range of 20–25% compared to the pre-pandemic period. The European Commission (2023) emphasizes that the aging of the population is one of the greatest challenges for future health expenditure. In 2023, 21% of the EU population was over 65 years of age, and this percentage is projected to reach almost 30% by 2050. At the same time, the EU has a shortage of more than 1.2 million medical professionals, and over a third of doctors and a quarter of nurses are over 55 years of age (European Commission, 2023). Although the pandemic has highlighted the importance of preventive healthcare, some countries have reduced spending in this area since 2021. For example, in Estonia, the share of prevention spending in total health expenditure fell from 8.8% in 2021 to 6.1% in 2022 (WHO, 2023b). The OECD recommends additional investments in prevention, as well as in improving the human resource structure, estimating that a permanent increase of at least 0.6% of GDP in public health expenditure would be needed (OECD, 2023). The Recovery and Resilience Facility (RRF) and the Next Generation EU Fund have been key in financing health reforms after the pandemic. For example, Italy has been allocated €194.4 billion and Spain €79.85 billion, a significant portion of which is allocated to health (The Times, 2022). However, differences in transparency and efficiency in the use of these funds have been observed across member states.
The increase in public spending on health during the COVID-19 pandemic has been one of the largest in the recent history of the European Union. However, after the initial wave of emergency financial measures, the question has arisen as to whether this level of spending will become structurally permanent or is a temporary phenomenon caused by the crisis. According to OECD (2023), in 2022 and 2023, there has been a slight decrease in total health expenditure as a percentage of GDP in most member states, indicating the end of a large number of temporary funding programmes. The share of health expenditure in GDP, although higher than before the pandemic, was lower compared to 2020 and 2021 (OECD, 2023). Eurostat (2023) notes a similar trend: in 2022, the share of public health expenditure in GDP was 8.1% on average in the EU, a decrease compared to the pandemic peak, but still higher compared to the period 2015–2019, when it was around 7.0% of GDP. This suggests that some of the increase has been maintained, but not to the full extent. Although some funding has been withdrawn, several countries have permanently increased salaries for health workers and invested in the digitalisation and modernisation of the system. For example, Finland, Estonia and France have maintained increased budgets for training, human resources policies and e-health, which is a signal of ongoing transformation (WHO, 2023; OECD, 2023). Mladovsky et al. (2022) state that the pandemic has stimulated structural investments that have in many cases continued even after the lifting of emergency measures, but warn that their sustainability will depend on long-term fiscal policy and political will. The European Commission (2023) points out that the durability of increased spending is conditioned by inflation, public debt and limited budgetary space, and that in some countries a rebalancing reduction in health spending has already been observed. In Italy and Spain, for example, despite an initial increase, some health items were reduced in 2023 in line with a more restrictive fiscal policy. According to the analysis of Greer et al. (2022), the durability of increased spending will depend on whether health is treated as an investment or as a cost. The authors conclude that without strong political signals, there is a risk that health systems will return to “pre-pandemic levels of financing that proved insufficient in the crisis”. Part of the increased public spending and for health it has become permanent — especially in areas such as salaries, human resources and digitalisation — but overall, health budgets have started to normalise. The sustainability of increased investments remains conditional on economic circumstances and political support for public health.
The COVID-19 pandemic has revealed significant weaknesses in the health systems of EU Member States, but has also become a catalyst for numerous reforms. Since 2021, many countries have started structural changes in the areas of financing, human resources policy, digitalisation, as well as strengthening the resilience of the systems. One of the most prominent reforms relates to the accelerated digitalisation of health services. According to the WHO report (2023), countries such as Estonia, Finland and the Netherlands have invested significantly in electronic health records, telemedicine and systemic exchange of health data. These investments have become a permanent part of the health infrastructure. The European Commission (2022) points out that more than 200 projects have been supported under the EU4Health programme, which aim to improve the digital connectivity and interoperability of health systems across the EU. Many countries have begun to reform the recruitment, education and retention of health workers. OECD (2023) indicates that countries such as Germany, Portugal and the Czech Republic have adopted new strategies to increase the number of nurses and doctors, including facilitating the recruitment of staff from other EU countries and increasing funding for medical education. Rechel et al. (2022) states that the crisis has shown that many health systems were understaffed, which has led to the adoption of long-term plans to increase employment and better allocate resources across regions. Within the framework of national recovery and resilience plans (Recovery and Resilience Facility – RRF), Member States have made significant investments in hospital infrastructure, equipment, laboratories and the public health sector. For example, Italy has invested more than €15 billion in the reconstruction of health institutions and the modernization of capacities (European Commission, 2023). Greer et al. (2023) note that the existence of the RRF mechanism has enabled the direct integration of health investments into economic policies, which represents the first significant step forward in financial coordination at the EU level in the field of health. After the pandemic, the capacity of institutions for prevention and management of health risks was strengthened. Mladovsky et al. (2022) point out that the system for monitoring the epidemiological situation and the procurement of medicines and vaccines was reorganized. The formation of HERA (Health Emergency Preparedness and Response Authority) in 2021 represents an EU institutional mechanism for rapid response to future crises.
The pandemic has left a deep mark on the structure and financing of health systems in EU member states. Reforms initiated in the post-crisis period show a tendency towards greater digitalization, better human resource management and more resilient institutions. Although the financial volume of investments is partially decreasing, their structure points to long-term systemic changes. The financing of health systems in the European Union after the COVID-19 pandemic remains heterogeneous, which is a consequence of historical, institutional and economic differences between member states. Differences are manifested in the sources of financing, the role of the state, the degree of centralization of the system, as well as priorities in the distribution of funds. EU member states use different models of health financing. Countries such as Germany, France and the Netherlands use the Bismarck model, based on compulsory health insurance and employer and employee contributions. In contrast, the United Kingdom, Sweden and Denmark use the Beveridge model, financed primarily from taxes and organized through centralized public services (Mossialos et al., 2017; OECD, 2023). In recent years, especially after the pandemic, some countries have introduced hybrid mechanisms — for example, the Czech Republic and Croatia have maintained insurance systems but increased budget transfers to cover the costs of the pandemic (Rechel et al., 2022). The share of public versus private financing varies considerably. For example, the public sector finances over 80% of total health expenditure in Sweden, France and Germany, while in Bulgaria and Latvia this percentage is below 70% (WHO, 2023). This imbalance significantly affects the accessibility and equity of services. Differences in the economic strength of countries are directly reflected in budgetary capacities.
Table 1: Differences in health financing policies among EU countries
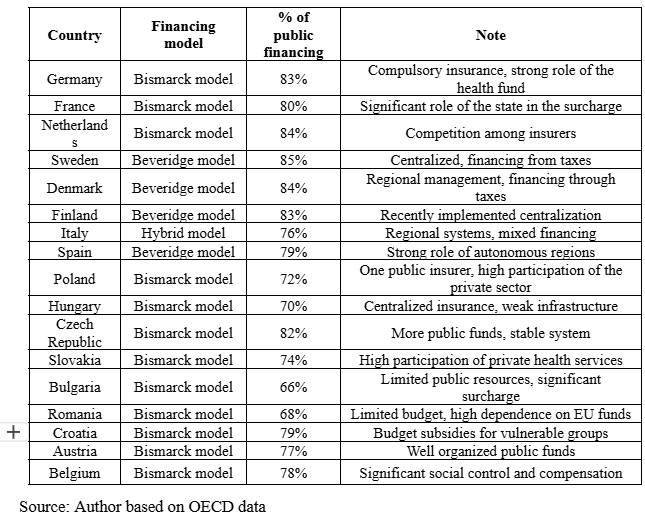
While countries such as Germany and the Netherlands were able to increase their health budgets in the short term and finance long-term measures, eastern member states, such as Romania or Slovakia, relied significantly more on European funds such as the RRF (European Commission, 2023; Eurofound, 2022). Political stability and institutional capacity play a key role. According to a study by Greer et al. (2023), countries with greater administrative efficiency and a tradition of intersectoral coordination (e.g. Scandinavia and Benelux) were better able to use the crisis as an opportunity for systemic reform. In contrast, countries with more unstable health policies were more likely to resort to ad hoc measures.
Analysis and discussion
The COVID-19 pandemic has led to a dramatic increase in public health spending in most European Union countries. According to OECD Health Statistics (2023), average health spending as a share of GDP in the EU rose from 8.8% in 2019 to 10.9% in 2020. However, after the pandemic, a gradual stabilization and decrease in the percentage is observed in 2022 and 2023 — on average to around 9.5%, which is still higher than before the pandemic (OECD, 2023; WHO, 2023). At the individual country level, Germany increased public health spending by more than €30 billion in 2020 during the pandemic, while in 2022 and 2023 some programs were abolished or reformed, but spending on long-term care, digitalization and system resilience remained high (Busse et al., 2022). A similar trend is observed in France, where spending increased to 12.3% of GDP in 2020–2021, before falling to around 11% in 2023 (OECD, 2023).
On the other hand, Eastern European countries such as Romania and Bulgaria did not have the fiscal strength to increase spending to the same extent, and relied heavily on European funds. Nevertheless, these countries also experienced a relative increase in health spending during the pandemic (Rechel et al., 2022), but after 2021 these figures declined more rapidly than in Western member states.
The structure of spending changed significantly during and after the pandemic. During the pandemic, expenditures for emergency supplies, hospital treatment, testing, vaccination and protective equipment dominate, while after 2021, expenditures for hospital modernization, digital infrastructure, staff recruitment and strengthening primary health care increase (European Commission, 2023; Eurofound, 2022).
Compared to the pre-pandemic period, the following changes are observed:
-
Average per capita expenditure in the EU increased from €2,887 (2019) to €3,528 (2021), and remained stable at €3,491 in 2023 (OECD, 2023).
-
The percentage of health expenditure in GDP in 2023 was still 0.7–1.2 percentage points higher than in 2019 in most Member States.
These trends suggest that some of the effects of the pandemic on health system financing have become structural, although with variations across countries.
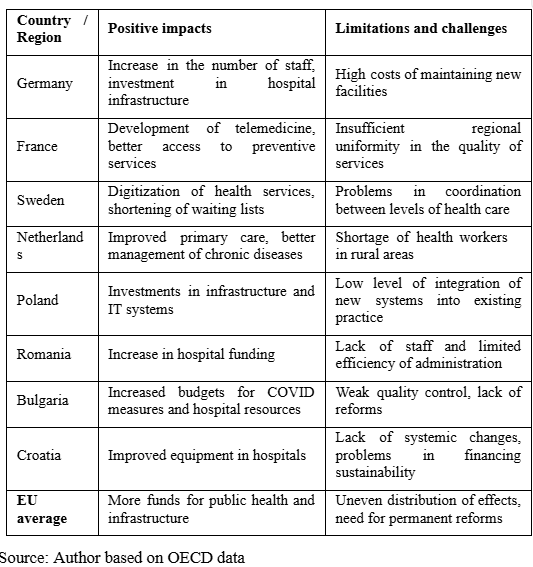
Increased public spending on health during and after the COVID-19 pandemic has had a significant impact on various aspects of the quality of health services in the European Union. Research suggests that the additional funds have led to improvements in some segments of the system, while at the same time revealing structural challenges that could not be solved by increasing the budget alone. According to the OECD (2023), additional financial resources have enabled accelerated recruitment of health personnel, improved hospital infrastructure and greater digitalization of services, which have contributed to better access and efficiency of treatment. For example, in Germany and the Netherlands, increased investment in primary health care has resulted in shorter waiting lists and greater availability of preventive services (OECD, 2023).
Table 2: Healthcare expenditure in selected EU countries (2019–2023)

In countries such as France and Sweden, a significant portion of the money has been directed towards digital health platforms and telemedicine, which has improved access to health services in rural and underserved areas (European Commission, 2022). Increased spending has also enabled better management of chronic diseases, which has been noted as a positive development in the analyses of the European Observatory on Health Systems (2023). However, studies show that higher financial allocations have not always led to proportional improvements in the quality of services. In Eastern European countries such as Bulgaria, Romania and Hungary, although there have been budget increases, systemic problems such as shortages of medical staff, inefficient allocation of resources and insufficiently reformed governance mechanisms have limited the effects of increased investments (Rechel et al., 2022). Short-term measures (such as one-off additional budget transfers) have not always accompanied strategic reforms, which has affected the sustainability of improvements. In many cases, there has been insufficient investment in staff training, which has limited the capacity to improve health outcomes (WHO, 2023).
Table 3: Impact of increased public spending on the quality of healthcare services in EU countries after the COVID-19 pandemic
The European Commission (2023) points out that despite initial investments in health through funds such as NextGenerationEU and RRF, fiscal consolidation in the coming years may threaten the continuity of financial support, especially in countries with high deficits. The sustainability of health financing is further burdened by demographic trends. According to WHO (2023), by 2050, more than 30% of the EU population will be over 65 years of age, which will lead to greater pressure on health and social services. The costs of chronic diseases, long-term care and pharmaceuticals are growing faster than total GDP, which raises the question of financial sustainability without additional reform measures (Mladovsky et al., 2022). Research by Rechel et al. (2022) and Greer et al. (2023) indicates that long-term sustainability depends on the efficiency of the system, and not only on the amount of investment. Examples such as Sweden and the Netherlands show that a combination of efficient governance, digitalization and a focus on primary and preventive care can result in better outcomes with more stable costs. In contrast, systems that rely on short-term budget interventions and lack clear cost control mechanisms (e.g. Bulgaria, Romania) risk failing to maintain post-pandemic service levels without new borrowing or cuts to other budget items.
Table 4: Overview of key factors influencing the long-term sustainability of increased health spending by region within the EU
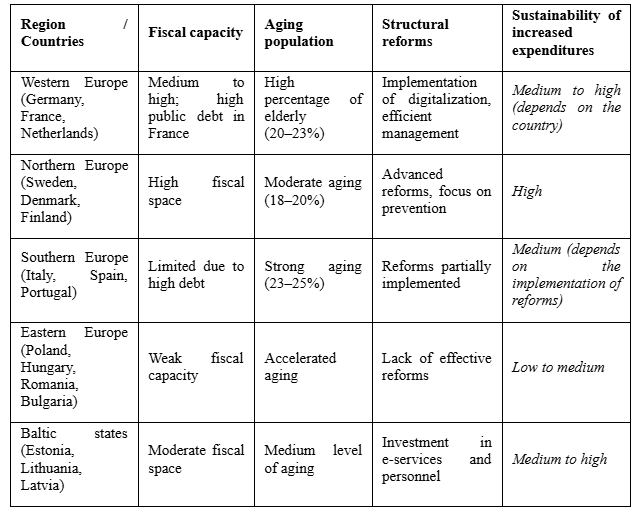
Source: Author based on data from OECD, WHO, and European Commission
The long-term sustainability of increased health budgets in the EU will depend on a combination of factors: macroeconomic conditions, political will, spending efficiency and population structure. Without deeper reforms in resource management, strengthening primary care and sustainable human resource development, maintaining high levels of financing will be a challenge for many countries.
Conclusion
A survey of public health spending in the EU during and after the COVID-19 pandemic shows that the pandemic has significantly changed the level, structure and dynamics of health system financing in most Member States. In 2020–2021, there were record increases in health budgets, both in absolute terms and as a share of GDP. For example, in Germany, health spending increased from 11.7% of GDP in 2019 to over 13% in 2020 (OECD, 2022). Similar trends were observed in France, Spain and Italy (Eurostat, 2023). The data show that these increases are largely the result of measures to combat the pandemic – the procurement of vaccines, tests, personal protective equipment, but also investments in intensive care capacities and workforce. Comparative analysis also points to differences between Western and Eastern EU member states, with Western countries having greater fiscal capacity to respond to the crisis (Rechel et al., 2021). One of the central conclusions is that adequate financing is not only a prerequisite for quality healthcare, but also for the resilience of the health system in times of crisis. Health systems with more stable budgetary frameworks and less reliance on emergency funds have managed to maintain better accessibility and continuity of services (WHO, 2021; Cylus et al., 2022). It is becoming increasingly clear that health budgets represent a strategic investment in social and economic security, and not just a cost. Financial stability enables capacity building, better resource management, and greater public trust in the system (Kluge et al., 2021; Bučalina Matić et al., 2024).
Based on the analysis and insights into the development of public health spending in the EU during and after the COVID-19 pandemic, the following recommendations can be formulated for creating more sustainable and resilient health systems:
-
Institutionalizing crisis funds and response mechanisms - EU Member States should develop sustainable mechanisms for financial response to health crises, as well as funds that will enable rapid mobilization of resources in future emergencies.
-
Improving the structure of public spending - It is recommended to focus on investments in primary health care, preventive measures and mental health, in order to reduce treatment costs in the long term and improve the overall health picture of the population.
-
Strengthening human resources and support for health workers - Increasing public spending must go hand in hand with investments in human resources - through better salaries, working conditions and continuous education.
-
Interoperability and digitalization - Investments in digital infrastructure and e-health should remain a priority, as they not only increase the efficiency, but also the resilience of health systems.
-
Regional cooperation and coordination within the EU - The pandemic has shown the importance of better coordination between Member States. Improving cooperation and sharing resources and information can significantly contribute to joint resilience.
Considering the dynamics of the health sector after the pandemic, future research should focus on:
-
A more detailed analysis of the effectiveness of new financing models introduced during and after the pandemic;
-
Comparing the impact of increased allocations on health outcomes in different countries;
-
Analyzing the contribution of European funds to the development of health systems in less developed EU Member States.
Reference
Beazley, I., de Carvalho, I. A., & Moreno-Serra, R. (2023). Public health financing and sustainability in post-pandemic Europe. Health Policy, 127(5), 558–567.
Bučalina Matić, A., Trifunović, D., & Blanuša, A. (2024). Značaj adekvatnog upravljanja otpadom i reciklaže u zaštiti životne sredine. Društveni horizonti, 3(7), 71–90. https://doi.org/10.5937/drushor2407071B
Bundesministerium für Gesundheit (BMG) (2021). Sondermittel für COVID-19-Bekämpfung.
Busse, R., Panteli, D., & Winkelmann, J. (2022). Germany: Health system review 2022. European Observatory on Health Systems and Policies.
Cylus, J., Panteli, D., van Ginneken, E. (2022). Addressing health system resilience in Europe: lessons from the COVID-19 pandemic. Eurohealth, 28(1), 3–8.
Ćulibrk, M. (2021). Javna potrošnja i finansiranje zdravstvenog sistema u Srbiji. Ekonomika zdravstva, 17(2), 45–59.
Eurofound (2022). Impact of COVID-19 on health services and health workforce in Europe. Luxembourg: Publications Office of the European Union.
European Commission (2021, 2022, 2023). EU4Health Programme 2021–2027. State of Health in the EU – Companion Report. Recovery and Resilience Scoreboard: Health investments overview. EU economic outlook and sustainability of healthcare spending. Publications Office of the European Union. Retrieved from: https://ec.europa.eu
European Court of Auditors (2021). EU Solidarity Fund support for COVID-19.
European Observatory on Health Systems and Policies (2023). Health system responses to the COVID-19 pandemic in the EU.
Eurostat (2020, 2021, 2022, 2023). General government expenditure by function (COFOG). Health care expenditure statistics. Government expenditure on health. Retrieved from https://ec.europa.eu/eurostat
Fattore, G., & Tediosi, F. (2022). Sustainability of increased public health expenditure in the EU: Lessons from COVID-19. Health Economics Review, 12(1), 56.
Greer, S. L., Jarman, H., & Baeten, R. (2022). EU health policy and the COVID-19 pandemic: From crisis to reform. Health Economics, Policy and Law, 17(2), 135–149.
Greer, S. L., Jarman, H., & Baeten, R. (2023). Health policy after COVID-19: Institutional resilience and reform in the EU. Health Economics, Policy and Law, 18(1), 89–104.
Greer, S. L., Jarman, H., & Baeten, R. (2023). Institutional capacity and sustainability in EU health systems. Health Policy, 127(3), 235–248.
Greer, S. L., Jarman, H., & Baeten, R. (2023). The politics of health system reform in the EU after COVID-19. Journal of Health Politics, Policy and Law, 48(1), 123–139.
Italian Ministry of Economy and Finance (2021). COVID-19 Budget Measures in Italy.
Jovanović, B., Ranitović, A. i Jevtić, M. (2018). Izvori finansiranja zdravstvene zaštite u Srbiji – analiza i komparativni pregled. Ekonomika, 64(2), 167–178.
Karanikolos, M., & Mossialos, E. (2020). Health systems resilience: Lessons from the COVID-19 pandemic in Europe. Eurohealth, 26(2), 7–12.
Kluge, H. H. P., Jakab, Z., Bartovic, J., D'Anna, V., & Severoni, S. (2021). Reflections on health-system responses to COVID-19 in the WHO European Region. The Lancet Regional Health–Europe, 1, 100021.
Kovačević, M., Pavlović, A. i Petrović, N. (2022). Finansijska podrška EU zdravstvenom sektoru Srbije tokom COVID-19 pandemije. Zdravstvena zaštita, 51(1), 65–72.
Kovačević, M., Pavlović, A. i Radovanović, I. (2021). Privremene i sistemske mere finansiranja zdravstva u Srbiji tokom pandemije COVID-19. Zdravstvena zaštita, 50(3), 211–219.
Mihaila, I., & Popescu, R. (2022). Romania's public health expenditure dynamics during COVID-19. Journal of Health Economics and Policy, 18(3), 211–225.
Ministarstvo zdravstva RH (2021). Izvješće o troškovima zdravstvenog sektora u kontekstu COVID-19 pandemije.
Ministère de la Santé (2021). Rapport annuel sur les dépenses de santé pendant la pandémie.
Mladovsky, P., Cylus, J., & Karanikolos, M. (2022). Public health spending during the COVID-19 pandemic in Europe: impact and sustainability. Health Policy, 126(4), 321–329.
Mladovsky, P., Cylus, J., & Thomson, S. (2022). Resilient and people-centred health systems in the EU: Lessons from COVID-19. Eurohealth, 28(2), 10–15.
Mossialos, E., Wenzl, M., Osborn, R., & Sarnak, D. (2018). International Profiles of Health Care Systems. The Commonwealth Fund.
OECD (2017, 2018, 2019, 2021, 2022, 2023). Health at a Glance: OECD Indicators. OECD Publishing, Paris.
Pajić, S., Lalić, G., Trifunović, D., Maltez, K., & Jovanović, P. (2025). The influence of social networks on the teaching process of language learning. Oditor, 11(3). https://doi.org/10.59864/Oditor22503SP
Pejić, A. i Matić, B. (2017). Struktura i trendovi javne potrošnje na zdravstvo u Srbiji. Ekonomika, 63(3), 273–288.
Rajan, S., Cylus, J., & McKee, M. (2021). Health system resilience: learning from the COVID-19 pandemic in Europe. Eurohealth, 27(1), 3–7.
Rechel, B., Jakubowski, E., & McKee, M. (2022). Health financing reforms in Europe after COVID-19. WHO Regional Office for Europe.
Rechel, B., Jakubowski, E., & McKee, M. (2022). Health Systems in Transition: Health financing reforms in Europe after COVID-19. European Observatory on Health Systems and Policies.
Rechel, B., Jakubowski, E., & McKee, M. (2022). Health workforce in Europe: A new agenda for policy action. European Observatory on Health Systems and Policies.
Rechel, B., Maresso, A., Sagan, A., & Hernandez-Quevedo, C. (2021). Organization and financing of public health services in Europe: Country reports. WHO Regional Office for Europe.
Rechel, B., Maresso, A., Sagan, A., & McKee, M. (2022). Health systems in transition: country reports. WHO Regional Office for Europe.
Reeves, A., Basu, S., McKee, M., & Stuckler, D. (2019). Financing health systems in Europe before COVID-19: an overlooked vulnerability. European Journal of Public Health, 29(6), 1046–1051.
Reeves, A., Basu, S., McKee, M., & Stuckler, D. (2022). COVID-19 and public health expenditure in Europe: Policy responses and economic impact. Health Policy, 126(5), 345–357.
Simić, S. i Petrović, V. (2019). Regionalne razlike u finansiranju zdravstva u Evropi: Izazovi i mogućnosti za Srbiju. Zdravstvena zaštita, 48(2), 145–152.
Simić, S., Petrović, V. i Jovanović, M. (2020). Izazovi finansiranja zdravstvenog sistema Srbije – analiza i predlozi mera. Zdravstvena zaštita, 49(2), 117–124.
Simić, S., Petrović, V. i Marić, G. (2018). Finansiranje zdravstvenog sistema Srbije u kontekstu evropskih integracija. Zdravstvena zaštita, 47(3), 165–172.
Stanković, B. i Kovačević, M. (2021). Finansiranje zdravstvenih sistema u uslovima pandemije COVID-19. Zdravstvena zaštita, 50(2), 119–127.
SURS (2022). Slovenian government expenditure on health during the pandemic.
The Times (2022). Draghi’s billions: How the EU is spending its COVID recovery cash. preuzeto sa: https://www.thetimes.co.uk
WHO - World Health Organization (2023b). Current health expenditure in 2022 back to business as usual. European Observatory on Health Systems and Policies.
WHO - World Health Organization. (2018, 2019, 2021, 2022, 2023). Public spending on health: A closer look at global trends. WHO, Geneva.
WHO - World Health Organization. (2023a). Estonia: Increased public health expenditure in 2023 highlights the impact of wage pressures. European Observatory on Health Systems and Policies.
Objavljeno u
Vol. 32 No. 1 (2026)
Ključne reči
Licenca
Ovaj rad je objavljen pod Creative Commons Attribution 4.0 International (CC BY 4.0).
Autori zadržavaju autorska prava nad svojim radom.
Dozvoljena je upotreba, distribucija i adaptacija rada, uključujući i u komercijalne svrhe, uz obavezno navođenje originalnog autora i izvora.
Zainteresovani za slična istraživanja?
Pregledaj sve članke i časopise